Ultrasound of Acute and Chronic Appendicitis
Appendicitis is one of the most common causes of acute abdominal pain requiring urgent surgical intervention. Ultrasound serves as an excellent first-line imaging modality, particularly in children, young adults, and pregnant individuals where minimizing radiation exposure is paramount.
Clinical Presentation
The clinical manifestation of appendiceal inflammation varies significantly depending on the temporal profile of the disease:
- Acute Appendicitis:
- Classic visceral periumbilical pain migrating over hours to somatic localization in the right lower quadrant (RLQ) / Right Iliac Fossa (RIF).
- Prominent anorexia, nausea, and emesis.
- Low-grade fever with progressive abdominal rebound tenderness, guarding, and rigidity at McBurney’s point.
- Chronic Appendicitis:
- Recurrent, intermittent, or persistent prolonged right lower quadrant pain.
- Smoldering clinical symptoms extending over weeks, months, or years.
- Typically presents without spiked pyrexia or systemic leukocytosis.
:::tip[Operator Performance Key] Ultrasound achieves a sensitivity of 75–90% and a specificity of 85–95% for acute appendicitis when performed by experienced operators using a systematic graded compression technique. :::
Ultrasound Findings
Acute Appendicitis
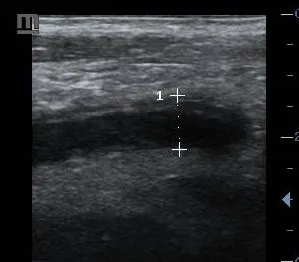
- A non-compressible tubular structure measuring > 6 mm in outer-to-outer diameter.
- The “Target sign” or “doughnut sign” in transverse views, demonstrating concentric, distinct hyper- and hypoechoic wall layers with a hypoechoic outer boundary matching the muscularis propria.
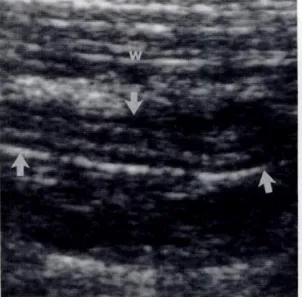
- Asymmetric or symmetric wall thickening (> 2–3 mm) displaying prominent active hyperemia on Color or Power Doppler assessment.
- Inflammatory splinting of periappendiceal fat, manifesting as structured, non-compressible, highly hyperechoic fat surroundings.
- An appendicolith (fecalith): An intraluminal, highly echogenic focus creating dense posterior acoustic shadowing.
- Periappendiceal free fluid or loculated reactive fluid pockets.
- Complex fluid collections indicative of macro-perforation and abscess formatting.
Chronic Appendicitis
- A fibrotic, irregularly thickened wall showing variable structural architecture and frequent focal loss of the normal multi-layered wall appearance.
- Muted periappendiceal fat stranding that is significantly less pronounced and less hyperemic than acute variations.
- Associated reactive lymphoid hyperplasia in neighboring structures.
- Minimal to absent color flow vascularity on low-flow Doppler controls, confirming a lack of acute active exudation.
- Focal mural strictures or secondary cystic-like dilatation of the distal appendiceal lumen.

Graded Compression Technique
Executing a high-yield appendiceal sonographic exam requires a strict, methodical approach:
- Position the patient supine and utilize a high-frequency linear array transducer (typically 5–12 MHz) to achieve optimal spatial resolution.
- Initialize scanning at the level of the ascending colon in the right upper quadrant, tracing inferiorly to cross-reference structural transitions.
- Locate the terminal ileum and the rigid psoas muscle bed to use as stable anatomic landmarks mapping the base of the cecum.
- Apply progressive, gradual downward pressure to slowly displace air-filled, overlying mobile large or small bowel loops while assessing the elasticity and compressibility of the structures.
- Continuously evaluate for direct and secondary inflammatory markers, switching to high-sensitivity Color or Power Doppler settings to screen for mural perfusion changes.
Diagnostic Criteria Comparison
| Diagnostic Feature | Acute Appendicitis | Chronic Appendicitis |
|---|---|---|
| Outer Diameter | Strictly > 6 mm | Variable configuration (frequently 5–7 mm) |
| Mural Wall Thickness | Echo measurements > 2–3 mm | > 2 mm with minimal interstitial edema |
| Concentric Wall Layers | Preserved anatomical architecture (Target Sign) | Often distorted, blunted, or structurally lost |
| Doppler Vascularity | Markedly increased (perimural hyperemia) | Mild, low-velocity, or entirely normal signals |
| Surrounding Mesenteric Fat | Dense, highly echogenic hyperechoic fat | Muted fat stranding without massive expansion |
| Compressibility Control | Entirely rigid and non-compressible | Fixed but can be partially compressible |
Differential Diagnosis
The clinician must actively differentiate appendiceal presentations from several other processes localized to the right lower quadrant:
- Mesenteric Adenitis: Clusters of enlarged, hyperemic, and tender mesenteric lymph nodes in the RIF with a completely normal, compressible appendix.
- Omental Infarction: An intensely painful, focal, non-compressible mass of hyperechoic fat directly beneath the abdominal wall layer, separate from the cecum.
- Right-Sided Colonic Diverticulitis: Focal outpouches and inflammatory thickening localized to the cecal or ascending bowel walls.
- Gynecological Pathologies: Ovarian cyst accidents (torsion/rupture), Pelvic Inflammatory Disease (PID) featuring pyosalpinx, or an unruptured/ruptured ectopic pregnancy.
- Crohn’s Disease: Transmural wall thickening localized to the terminal ileum, showcasing classic mucosal skip lesions.
- Typhlitis (Neutropenic Enterocolitis): Severe circumscribed cecal and ascending colonic mural thickening identified in immunocompromised populations.
Conclusion
Ultrasound remains an indispensable first-line diagnostic method for triage in suspected cases of appendicitis, offering quick and definitive confirmation without the penalty of ionizing radiation. Accurate discrimination between acute and chronic variants rests on careful quantification of outer diameter boundaries, analysis of preserved or altered wall layers, mapping of perimural color Doppler tracks, and evaluating adjacent mesenteric fat reactions. Direct integration of these strict ultrasound parameters with bedside clinical signs ensures high diagnostic sensitivity.
References
- Puylaert JB. Acute appendicitis: US evaluation using graded compression. Radiology. 1986;158(2):355-360.
- Kessler N, et al. Appendicitis: evaluation of sensitivity, specificity, and predictive values of US, Doppler US, and laboratory findings. Radiology. 2004;230(2):472-478.
- Trout AT, et al. Imaging of acute appendicitis in children: AJR Expert Panel Narrative Review. AJR Am J Roentgenol. 2022;219(2):204-214.
- Mostbeck G, et al. How to diagnose acute appendicitis: ultrasound first. Insights Imaging. 2016;7(2):255-263.