Appendicitis: Imaging Diagnosis
Appendicitis is the most common abdominal surgical emergency worldwide, carrying a lifetime risk of approximately 7%. Imaging plays a crucial role in securing an accurate diagnosis, particularly in patients presenting with atypical clinical manifestations. This article details the characteristic diagnostic features of appendicitis across multiple imaging modalities, focusing on high-frequency ultrasound as the first-line evaluation in children and pregnant individuals, and contrast-enhanced Computed Tomography (CT) as the gold standard for adult populations.
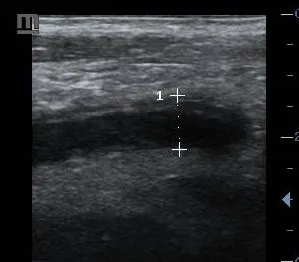
1. Ultrasound Features
Graded compression ultrasound stands as the initial imaging modality of choice for pediatric and pregnant patients presenting with suspected acute appendicitis to eliminate the risks associated with ionizing radiation.
Examination Technique
The study is performed utilizing a high-frequency linear array transducer (5–12 MHz). The examiner applies steady, gradual compression across the right lower quadrant (RLQ) to displace overlying gas-filled loops of bowel, minimize the distance to the retroperitoneum, and clearly isolate the appendiceal structure against stable anatomical benchmarks.
Diagnostic Criteria
- A non-compressible tubular structure possessing an outer wall-to-outer wall diameter exceeding 6 mm.
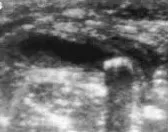
- The classic “Target sign” visualized in the transverse scanning plane, showing concentric alternating layers of tissue.
- Mural wall thickening exceeding 3 mm combined with prominent localized hyperemic flow on Color or Power Doppler interrogation.
- Increased hyperechogenicity of periappendiceal mesenteric fat, reflecting active regional inflammatory extension.
- An appendicolith (fecalith): Identified as an intraluminal, highly reflective echogenic focus generating distinct posterior acoustic shadowing.
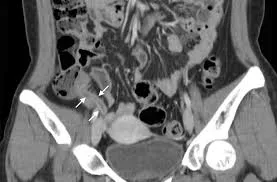
2. CT Features
Contrast-enhanced Multi-Detector Computed Tomography (MDCT) represents the diagnostic gold standard for evaluating suspected appendicitis in adults, achieving a sensitivity of 94–98% and a specificity of 95%.
Imaging Protocol
Scans should be acquired on a multi-detector system utilizing intravenous contrast enhancement (iodinated contrast medium) timed for the portal venous phase. Oral or rectal contrast administration remains optional. Images should be reconstructed in thin axial sections (2–3 mm) alongside coronal and sagittal multiplanar reformations.
Diagnostic Criteria
- Appendiceal diameter exceeding 6 mm associated with circumferential wall thickening and luminal distension.
- Periappendiceal fat stranding: Increased attenuation and linear haziness in the surrounding fat layers; this stands as the most sensitive secondary sign of acute inflammation.
- Abnormal mural enhancement: Intense or asymmetric enhancement of the appendiceal wall following intravenous contrast administration.
- An appendicolith: A high-attenuation, calcified intraluminal focus easily differentiated on non-contrast or contrast reconstructions.
- Adjacent fascial thickening: Inflammatory thickening of the lateroconal fascia or the parietal peritoneum.
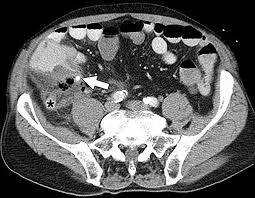
3. Complicated Appendicitis
Identifying imaging features of complicated appendicitis—such as macro-perforation, phlegmon, or localized abscess formation—is critical, as these findings often alter the surgical or clinical approach.
Key Imaging Findings
- Focal defect in the enhancing appendiceal wall: The most direct and definitive sign of structural wall perforation.
- Extraluminal free air bubbles: Localized micro-pneumoperitoneum adjacent to the appendiceal tip (generalized pneumoperitoneum is rare).
- Phlegmon formation: An ill-defined, highly inflammatory non-contained soft tissue mass in the right iliac fossa.
- Appendiceal abscess: A well-circumscribed, loculated fluid collection demonstrating a thick, prominently irregular rim of peripheral contrast enhancement.
- Extensive pelvic or lower abdominal free fluid containing low-level internal echogenic debris or complex fluid-debris lines.
Management Implications
Stable patients demonstrating contained perforations or mature abscess cavities are often managed initially via image-guided percutaneous drainage and targeted antibiotic therapy, followed by a delayed interval appendectomy. Conversely, patients with uncontained free perforation or diffuse peritonitis require immediate emergent surgical intervention.


4. Differential Diagnosis
Several acute gastrointestinal, mesenteric, and genitourinary pathologies can closely mimic the clinical and radiological presentation of appendicitis.
Common Clinical and Radiographic Mimickers
- Mesenteric Adenitis: Characterized by a cluster of enlarged, hyperemic, and tender mesenteric lymph nodes in the right lower quadrant, in the presence of a completely normal, compressible appendix.
- Omental Infarction: Presents as a focal, well-circumscribed mass of fat-attenuation showing irregular inflammatory stranding located directly beneath the anterior abdominal wall, lacking connection to the appendix.
- Acute Colonic Diverticulitis: Typically localized to the left side (sigmoid colon), but right-sided cecal or ascending colonic diverticulitis can present identically in older individuals or specific populations.
- Gynecological Pathologies: Conditions such as acute ovarian torsion, Pelvic Inflammatory Disease (PID) with tubo-ovarian abscesses, or a ruptured ectopic pregnancy must be excluded in female patients of childbearing age.
- Crohn’s Disease: Demonstrates marked, continuous, transmural wall thickening and hyperemia isolated to the terminal ileum, often with associated skip lesions.

5. Special Populations
Pediatric Considerations
Pediatric patients present with a significantly higher rate of appendiceal perforation (15–30%) due to delays in communication and a thin appendiceal wall. High-frequency ultrasound remains the mandated first-line modality to completely avoid radiation exposure. Operators should note that some pediatric criteria suggest an adjusted diagnostic cutoff diameter (> 5.5 mm).
Pregnancy Considerations
As gestation progresses, the growing gravid uterus progressively displaces the appendix superiorly and laterally, moving it out of the right lower quadrant toward the right upper quadrant or flank. Graded compression ultrasound is the initial study of choice. If ultrasound findings are indeterminate, non-contrast Pelvic/Abdominal Magnetic Resonance Imaging (MRI) is recommended as the next diagnostic step. CT imaging is strictly reserved for complex, highly suspicious clinical presentations after the first trimester.
Elderly Considerations
Elderly individuals frequently present with vague, atypical clinical signs (e.g., absence of spiked fever or localized rebound tenderness), often resulting in diagnostic delays and higher perforation rates at initial presentation. Furthermore, the presence of an underlying cecal or appendiceal malignancy must always be considered as an alternate primary diagnosis in this demographic.
Comparative Imaging Features
| Diagnostic Parameter | Ultrasound Evaluation | Computed Tomography (CT) |
|---|---|---|
| Appendiceal Diameter | > 6 mm, structurally rigid and non-compressible | > 6 mm absolute diameter cutoff |
| Mural Wall Thickness | > 3 mm with prominent internal color hyperemia | Thickened wall showing dense contrast enhancement |
| Surrounding Tissue | Hyperechoic, brightly inflamed mesenteric fat | Prominent periappendiceal fat stranding lines |
| Impacted Appendicolith | Highly echogenic focus generating sharp acoustic shadow | High-attenuation, calcified intraluminal focus |
| Perforation Sign | Localized wall layer disruption, fluid collections | Direct mural gap, free extraluminal gas bubbles |
References
- Pinto Leite N, Pereira JM, Cunha R, Pinto P, Sirlin C. CT evaluation of appendicitis and its complications: imaging techniques and key diagnostic findings. AJR Am J Roentgenol. 2005;185(2):406-417. doi:10.2214/ajr.185.2.01850406
- Doria AS, Moineddin R, Kellenberger CJ, et al. US or CT for Diagnosis of Appendicitis in Children and Adults? A Meta-Analysis. Radiology. 2006;241(1):83-94. doi:10.1148/radiol.2411050913
- Mostbeck G, Adam EJ, Nielsen MB, et al. How to diagnose acute appendicitis: ultrasound first. Insights Imaging. 2016;7(2):255-263. doi:10.1007/s13244-016-0469-6
- Kessler N, Cyteval C, Gallix B, et al. Appendicitis: evaluation of sensitivity, specificity, and predictive values of US, Doppler US, and laboratory findings. Radiology. 2004;230(2):472-478. doi:10.1148/radiol.2302021520
- Barger RL, Nandalur KR. Diagnostic performance of magnetic resonance imaging in the detection of appendicitis in adults: a meta-analysis. Acad Radiol. 2010;17(10):1211-1216. doi:10.1016/j.acra.2010.05.010
- Birnbaum BA, Wilson SR. Appendicitis at the millennium. Radiology. 2000;215(2):337-348. doi:10.1148/radiology.215.2.r00ma24337
- van Randen A, Bipat S, Zwinderman AH, Ubbink DT, Stoker J, Boermeester MA. Acute appendicitis: meta-analysis of diagnostic performance of CT and graded compression US related to prevalence of disease. Radiology. 2008;249(1):97-106. doi:10.1148/radiol.2483071652
- Drake FT, Mottey NE, Farrokhi ET, et al. Time to Appendectomy and Risk of Perforation in Acute Appendicitis. JAMA Surg. 2014;149(8):837. doi:10.1001/jamasurg.2014.77
- Rosen MP, Ding A, Blake MA, et al. ACR Appropriateness Criteria® Right Lower Quadrant Pain-Suspected Appendicitis. J Am Coll Radiol. 2011;8(11):749-755. doi:10.1016/j.jacr.2011.07.010
- American Institute of Ultrasound in Medicine (AIUM). AIUM practice guideline for the performance of ultrasound examinations of the abdomen and/or retroperitoneum. J Ultrasound Med. 2021;40(7):E1-E16. doi:10.1002/jum.15607