Appendix Ultrasound
High-resolution ultrasound stands as the primary diagnostic imaging modality for evaluating patients with suspected appendicitis. This non-invasive tool is especially crucial in pediatric populations, young adults, and pregnant individuals due to its excellent diagnostic accuracy and complete absence of ionizing radiation.
Appendiceal Anatomy
- Anatomic Location: The worm-like appendix vermiformis arises from the posteromedial aspect of the cecum, roughly 2 cm inferior to the ileocecal valve, and is typically localized in the right lower quadrant (RLQ).
- Normal Sonographic Characteristics:
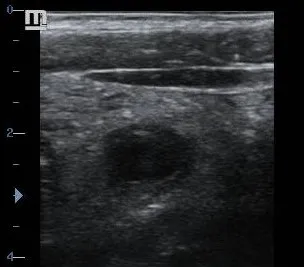
- Appears as a blind-ending, tubular structure in longitudinal sections and a concentric “target” ring in cross-section.
- Outer wall-to-outer wall diameter measures strictly < 6 mm.
- Individual wall thickness measures < 3 mm.
- Readily compressible under direct transducer footprint pressure.
- Free from surrounding hyperemic or hyperechoic mesenteric fat changes.
- Demonstrates completely absent or minimal intraluminal or mural flow signals on power Doppler imaging.
- Positional Variations: Positional deviations are common, with retrocecal localization representing the most frequent configuration. Pelvic, retroileal, preileal, and subhepatic positions can also occur, altering localized clinical signs.
Clinical Indications
1. General Indications
- Acute or intermittent localized right lower quadrant (RLQ) abdominal pain.
- Clinical evaluation for suspected acute appendicitis.
- Scanning and follow-up monitoring of known appendiceal abscess formations.
- Triage of non-specific or undifferentiated pediatric abdominal pain.
- Triage of pregnant individuals presenting with symptoms in the right lower quadrant.
2. Anatomic and Clinical Presentations
- Classic Inflammatory Appendicitis: Onset of visceral periumbilical distress that progressively migrates to somatic localization in the RLQ, associated with direct rebound tenderness and muscular guarding.
- Atypical Appendiceal Positions: Deep pelvic, flank, or diffuse generalized abdominal pain patterns resulting from retrocecal or pelvic locations.
- Pediatric Presentations: Variable, non-specific abdominal signs often presenting primarily as anorexia, uncontained emesis, and low-grade pyrexia.
Scanning Technique
1. Patient Preparation
- No dietary fasting or specialized fluid preparation is required. Immediate scanning should proceed for acute presentations.
- Patient Positioning: Place the patient in a standard flat supine position. Utilizing a slight left lateral decubitus tilt can help shift overlying gas-filled loops of small bowel medially.
- Patient Communication: Clearly explain the purpose of the exam, as the graded compression method can briefly exacerbate pain over inflamed areas.
2. System Optimization
- Transducer Selection: Use a high-frequency linear array transducer (7–15 MHz) to provide the near-field spatial resolution needed to evaluate mural layers.
- Depth Adjustment: Optimize the display depth to encompass the anterior psoas muscle margin and the external iliac vessel tracks.
- Harmonic Imaging: Enable tissue harmonics to suppress clutter artifacts and maximize contrast differences within the bowel walls.
- Doppler Configuration: Set low Pulse Repetition Frequency (PRF) limits (500–1000 Hz) and high wall filters to isolate low-velocity microvascular mural hyperemia.
3. Systematic Scanning Method
- Place the transducer over the localized point of maximal tenderness, which typically corresponds with McBurney’s point.
- Apply a graded compression technique, exerting slow, steady downward pressure. This displaces compressible, gas-filled cecal or ileal loops and thins the tissue layer without causing structural trauma.
- Isolate the internal psoas muscle belly, the crossing external iliac vessels, and the fluid-filled cecum to anchor the anatomical field.
- Locate the terminal ileum and trace it directly to its junction with the cecum to systematically map the appendiceal base.
- Trace the appendix along its entire length, scanning through both transverse and longitudinal axes from the cecal origin to its blind-ending tip to avoid missing isolated tip appendicitis.
Normal Sonographic Findings
A normal appendix presents as a tiny, compressible, blind-ending tube showing no reactive fluid or inflammatory alterations in the adjacent soft tissues. The surrounding mesenteric fat layers should remain uniformly thin and normal in echogenicity, displaying crisp, unhindered peristaltic motion in neighboring loops of bowel.
Pathological Findings
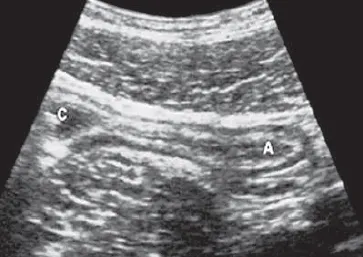
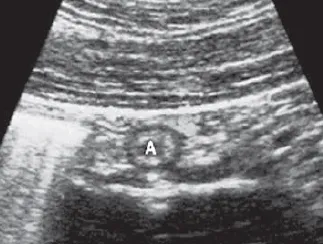
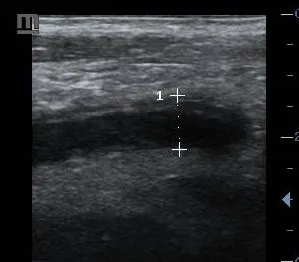
1. Acute Appendicitis
- Primary Diagnostic Signs: A rigid, non-compressible, blind-ending tubular structure demonstrating an outer wall-to-outer wall diameter > 6 mm, a thickened mural profile (> 3 mm), and prominent global wall hyperemia on color Doppler.
- Secondary Diagnostic Signs: Increased hyperechogenicity and splinting of the periappendiceal mesenteric fat, reactive localized free fluid collections, and an impacted calcified appendicolith producing sharp posterior acoustic shadowing.
2. Perforated Appendicitis
Characterized by a focal or diffuse disruption in the echogenic lines of the appendiceal wall. This structural break is often accompanied by a rapid decrease in luminal tension, the formation of complex periappendiceal fluid pockets, intense regional tissue reactions, and pocketed loculations of extraluminal gas bubbles.
3. Appendiceal Abscess
Presents as a complex, poorly defined fluid collection positioned immediately adjacent to the cecal tip or retrocecal space. The collection displays thick, irregular walls with increased peripheral vascularity, internal echogenic debris or septations, pocketed gas bubbles, and frequently contains a displaced or free appendicolith.
4. Mucocele of the Appendix
A distinct clinical entity presenting as a significantly distended, fluid-filled appendix completely lacking active inflammatory changes or perimural fat hyperemia. The outer diameter typically expands beyond 15 mm, and the lumen is filled with fine, onion-skin layers of echogenic mucin. Faint, irregular mural calcifications may also be present.
5. Appendiceal Neoplasms
- Neuroendocrine (Carcinoid) Tumors: Typically present as a well-circumscribed, homogenous hypoechoic nodule nestled at the appendiceal tip, often preserving the upstream wall layers.
- Adenocarcinoma: Manifests as an irregular, destructive mural mass or asymmetric wall thickening with complete loss of the distinct concentric wall layers and local infiltration.
- Metastatic Disease: A rare presentation characterized by nodular serosal distortion, typically originating from primary malignancies in the ovaries or upper gastrointestinal tract.



References
- American College of Radiology (ACR). (2023). ACR Appropriateness Criteria® Right Lower Quadrant Pain. Journal of the American College of Radiology, 20(1S), S78-S92.
- Puylaert, J. B. (2022). Ultrasonography of the Acute Abdomen (2nd ed.). Springer.
- Rumack, C. M., & Levine, D. (2021). Diagnostic Ultrasound (6th ed.). Elsevier.
- World Society of Emergency Surgery (WSES). (2023). Guidelines for diagnosis and treatment of acute appendicitis. World Journal of Emergency Surgery, 18(1), 1-25.
- European Society of Pediatric Radiology (ESPR). (2022). Imaging guidelines for pediatric appendicitis. Pediatric Radiology, 52(3), 425-438.