Gastrointestinal Ultrasound: Complete Guide to Bowel Pathology
Gastrointestinal (GI) ultrasound has become increasingly valuable for evaluating acute and chronic bowel pathologies. High-resolution equipment enables detailed transabdominal visualization of fine tissue layers, serving as an outstanding, radiation-free diagnostic modality.
Gastrointestinal Anatomy
The Sonographic “Gut Signature”
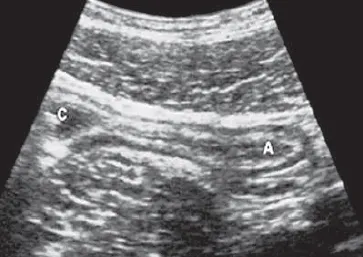
The healthy gastrointestinal tract displays a characteristic multi-layered appearance known as the gut signature. In high-frequency scans, the bowel wall resolves into five distinct, alternating hyperechoic and hypoechoic layers (from the lumen outward):
- Mucosa (Interface): Hyperechoic inner layer representing the contact interface between the luminal contents and the mucosal surface.
- Mucosa (Deep / Muscularis mucosae): Hypoechoic layer corresponding to the deep lamina propria and mucosal muscle boundary.
- Submucosa: Thick, prominent hyperechoic layer rich in connective tissues and vascular networks.
- Muscularis Propria: Hypoechoic layer corresponding to the smooth muscle coat (circular and longitudinal fibers).
- Serosa / Adventitia: Thin, sharp hyperechoic outer margin blending into the surrounding mesenteric fat.
Normal Wall Measurements
To avoid false-positive interpretations, wall thickness should be evaluated on the anterior wall segment of a moderately distended loop:
- Stomach Wall: < 5 mm
- Small Bowel Wall: < 3 mm
- Colonic Wall: < 4 mm
Clinical Indications
1. Primary Clinical Triggers
- Evaluation of acute, localized, or diffuse abdominal pain.
- Clinical suspicion of acute appendicitis or localized appendiceal abscess formation.
- Assessment, staging, and monitoring of Inflammatory Bowel Disease (IBD).
- Clinical signs of mechanical small or large bowel obstruction.
- Suspected intestinal intussusception (frequently in pediatric cohorts).
2. Specific Pathological Correlates
- Appendicitis: Acute right lower quadrant (RLQ) pain paired with localized rebound tenderness and guarding.
- Crohn’s Disease: Chronic, unremitting abdominal pain associated with systemic diarrhea, weight loss, and low-grade pyrexia.
- Mechanical Obstruction: Progressively worsening abdominal distension, obstipation, and bilious vomiting.
- Intussusception: Paroxysmal, colicky abdominal pain accompanied by palpable mass formations and classic “red currant jelly” stools.
Scanning Technique
1. Patient Preparation
- Fasting Protocol: A restriction of oral intake for 4–6 hours is required for upper gastrointestinal track examinations (stomach and duodenum) to minimize luminal gas volume and limit confusing postprandial fluid collections. Fasting is optional for emergent lower quadrant evaluations.
- Water-Fill Technique: Consuming 300–500 mL of degassed water can optimize evaluation of the gastric wall layers by forming an acoustic window.
- Patient Positioning: Initialize scanning with the patient flat supine, then utilize left lateral decubitus, right lateral decubitus, or erect postures as required to displace mobile bowel loops.
2. System Optimization
- Transducer Configuration: Use high-frequency linear array transducers (7–15 MHz) to resolve near-field wall layers. Lower frequency curvilinear probes (3–5 MHz) are reserved for deeply seated loops or heavily built patients.
- Tissue Harmonics: Enable harmonic imaging to eliminate artifactual internal echo fill-in and improve border definitions.
- Doppler Parameters: Optimize color flow settings with low Pulse Repetition Frequency (PRF) parameters (500–1000 Hz) to maintain high sensitivity for slow capillary wall perfusion.
3. Systematic Scanning Approach
- Graded Compression Method: Apply progressive, steady downward pressure over the area of interest. This technique slowly displaces compressible, gas-filled loops of small bowel, thins out the abdominal wall, and holds pathogenic structures fixed against the posterior muscular bed.
- Anatomic Tracking: Systematically track fixed landmarks such as the ascending colon, descending colon, terminal ileum, psoas muscle margins, and iliac vessels.
- Dynamic Analysis: Assess the presence, direction, and speed of active peristalsis alongside structural compressibility.
Normal Sonographic Findings
In a standard scan, high-resolution linear probes clearly map the five distinct structural layers of the gut signature. Small bowel loops should exhibit brisk, coordinated peristalsis, while colonic segments are readily differentiated by their non-peristaltic configurations and classic haustral configurations.

Pathological Findings
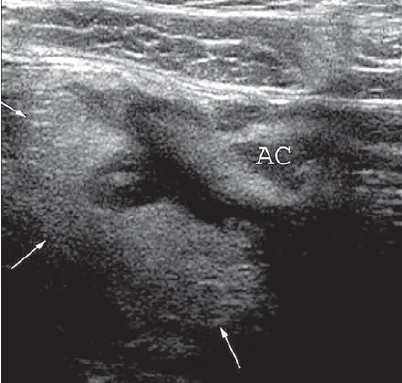
1. Acute Appendicitis
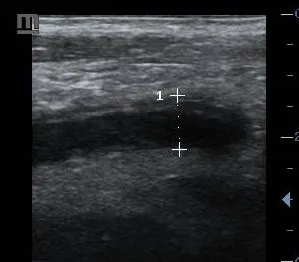
- Sonographic Presentation: A non-compressible, rigid, blind-ending tubular structure exceeding 6 mm in overall outer diameter.
- Key Findings: Circumferential wall thickening (> 3 mm), distinct target-sign configuration on cross-section, localized hyperemic wall perfusion on Doppler, and bright, hyperechoic inflammatory fat splinting.
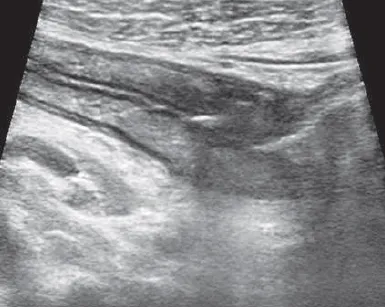
2. Inflammatory Bowel Disease (IBD)
- Crohn’s Disease: Characterized by segments of marked transmural wall thickening (> 4 mm), loss of normal layer stratification, local wall rigidity, skipped distribution patterns, and surrounding fibrofatty proliferation (“creeping fat”). Complications include transmural fistulous tracts and pocketed perienteric abscesses.
- Ulcerative Colitis: Diffuse, continuous, symmetrical wall thickening typically isolated to the colonic mucosa and submucosa, preserving the deeper muscular layers.
3. Bowel Obstruction
- Mechanical Small Bowel Obstruction: Characterized by dilated proximal small bowel loops (> 3 cm from outer margin) showing stretched, thin walls, fluid loading, and ineffective hyperperistalsis (“to-and-fro” motion), alongside completely collapsed distal loops.
- Paralytic (Adynamic) Ileus: Diffuse, uniform fluid and gas loading throughout both small and large bowel networks, accompanied by completely absent or akinetic peristaltic activity.
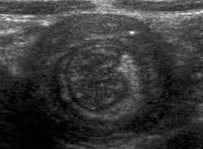
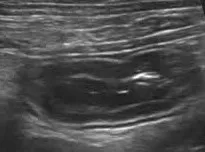
4. Intussusception
The invagination of a proximal segment of bowel (intussusceptum) into an adjacent distal segment (intussuscipiens).
- Transverse Plane: Appears as the pathognomonic “target sign” or “doughnut sign”, characterized by multiple concentric rings surrounding a central core of hyperechoic mesenteric fat.
- Longitudinal Plane: Displays the classic “pseudokidney sign”, where layered loops of bowel mimic a renal silhouette.
5. Acute Diverticulitis
Focal bowel wall thickening centered directly around a herniated outpocketing. The inflamed diverticulum presents as an out-pouching containing a highly hyperechoic fecalith that creates dense posterior shadowing. This is accompanied by intense hyperechoic pericolic fat reactions and variable peridiverticular microabscesses.
6. Neoplastic Processes
- Gastrointestinal Stromal Tumors (GIST): Well-circumscribed, hypoechoic exophytic or intramural masses originating from the deep muscularis propria layer, frequently displaying central necrotic cavities and prominent intrinsic vascular tracking.
- Adenocarcinoma: Manifests as a short-segment, irregular, eccentric hypoechoic wall thickening that completely destroys normal layer stratification, producing a fixed, rigid lumen (“apple-core” appearance).
- Bowel Lymphoma: Striking, bulky hypoechoic mural expansion that can cause atypical aneurysmal luminal dilatation while keeping the underlying layer definitions subtly visible.

References
- American College of Radiology (ACR). (2023). ACR Appropriateness Criteria® Right Lower Quadrant Pain. Journal of the American College of Radiology, 20(1S), S78-S92.
- Kratzer, W., et al. (2022). Atlas of Gastrointestinal Ultrasound (2nd ed.). Thieme.
- Nylund, K., et al. (2021). EFSUMB Recommendations for Gastrointestinal Ultrasound. Ultraschall in der Medizin, 42(3), 261-279.
- Wilson, S. R. (2022). The Gastrointestinal Tract. In: Rumack, C. M., & Levine, D. (Eds.), Diagnostic Ultrasound (6th ed., pp. 345-412). Elsevier.
- European Society of Gastrointestinal and Abdominal Radiology (ESGAR). (2023). Consensus Guidelines on Bowel Ultrasound in Inflammatory Bowel Disease. European Radiology, 33(1), 255-270.