Hepatic Candidiasis: Ultrasound Diagnosis & Management
Hepatic candidiasis, also called hepatosplenic candidiasis or chronic disseminated candidiasis, is a manifestation of systemic fungal infection most commonly seen in immunocompromised patients. Ultrasound plays a crucial role in early detection and monitoring of these fungal microabscesses.
:::note[Key Risk Factors]
- Neutropenic patients (especially post-chemotherapy)
- Hematologic malignancies (leukemia, lymphoma)
- Prolonged antibiotic use
- Stem cell transplant recipients :::
The characteristic “bull’s-eye” or “wheel-within-wheel” lesions are best visualized on ultrasound during the recovery phase when neutrophils return, which can sometimes correspond with a paradoxical clinical worsening.
Ultrasound Features
Hepatic candidiasis demonstrates evolving sonographic patterns based on the stage of the disease:
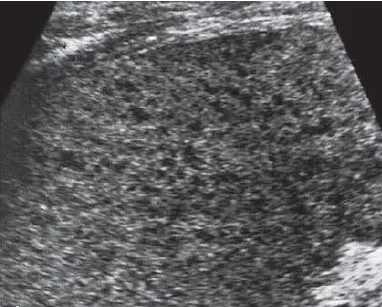
Early stage (Neutropenic phase): Subtle hypoechoic lesions (2 to 5 mm) with poorly defined margins. May be occult on ultrasound.

Classic 'Bull's-eye' Lesions: Central hyperechoic nidus surrounded by an intermediate hypoechoic ring and an outer hyperechoic rim.
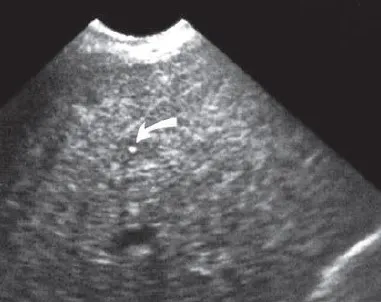
After Medical Therapy: Dense echogenic scar or calcification pattern visualized after successful medical treatment.
Diagnostic Pearls
- Timing matters: Lesions become significantly more visible as neutrophils recover.
- Size range: Typically 3 to 20 mm in diameter.
- Distribution: Random, diffuse, and often numerous, frequently presenting with greater than 10 separate lesions.
Differential Diagnosis
| Condition | Key Differentiating Features |
|---|---|
| Pyogenic abscess | Larger (greater than 2 cm), thick-walled, internal gas or air bubbles may be present |
| Metastases | Variable appearance, often larger, history of a known primary malignancy |
| Lymphoma | Diffuse infiltrative pattern, systemic hepatosplenomegaly, prominent adenopathy |
| Sarcoidosis | Non-calcified hypoechoic nodules, often accompanied by characteristic lung findings |
:::note[Clinical Clues to Diagnosis]
- Persistent fever despite broad-spectrum antibiotics in a neutropenic patient.
- Rising serum alkaline phosphatase with relatively normal bilirubin levels.
- Simultaneous splenic involvement is highly common (present in up to 80 percent of cases).
- Blood cultures are positive in only about 50 percent of cases. :::
Management Implications
1. Monitoring Treatment Response
- Lesions may initially appear to increase in size with immune reconstitution.
- Expect a gradual decrease in both number and size over weeks to months.
- Complete visual resolution on ultrasound can take anywhere from 6 to 12 months.
2. Recommended Follow-up Protocol
- Establish Baseline (At Diagnosis): Perform a complete baseline abdominal ultrasound as soon as systemic fungal infection is clinically suspected.
- Acute Surveillance (Every 2-4 Weeks): Repeat the scan every 2 to 4 weeks during the acute phase of medical treatment to document treatment response or rule out early confluence.
- Stabilization Checks (Monthly): Continue scan monitoring on a monthly interval until the active lesions completely stabilize, calcify, or fully resolve.
- Complication Screening (As Needed): Actively scan for secondary complications, such as large pyogenic bacterial abscess formation or macro-necrosis.
3. Antifungal Treatment Options
- First-line therapies: Echinocandins (such as caspofungin or micafungin).
- Alternative therapies: Liposomal amphotericin B or voriconazole.
- Duration: Treatment typically continues for 2 to 4 weeks after complete imaging resolution of the active lesions.