Bowel Obstruction Ultrasound
Bowel obstruction is a common surgical emergency where ultrasound serves as an excellent first-line imaging modality due to its real-time assessment capability, lack of radiation, and ability to evaluate peristalsis[cite: 1]. This article covers the sonographic features of different types of bowel obstruction with emphasis on distinguishing mechanical obstruction from paralytic ileus and identifying closed loop obstruction[cite: 1].
Key Advantages of Ultrasound
- Real-time evaluation: Critical for differentiating mechanical vs paralytic obstruction by observing peristalsis[cite: 1].
- No ionizing radiation: Safe for repeated examinations in pediatric and pregnant patients[cite: 1].
- Bedside availability: Essential for unstable patients[cite: 1].
- Complication detection: Identifies extraluminal findings like free fluid or abscesses[cite: 1].
- Dynamic assessment: Compression allows evaluation of bowel loop distensibility[cite: 1].
1. Mechanical Small Bowel Obstruction (SBO)
Results from physical blockage of the intestinal lumen, most commonly due to adhesions (60%), hernias (15%), or neoplasms (15%)[cite: 1].
Pathophysiology
Obstruction leads to proximal bowel distension, fluid/air accumulation, and increased intraluminal pressure, which can compromise venous return, leading to ischemia and potentially perforation[cite: 1].
Ultrasound Findings
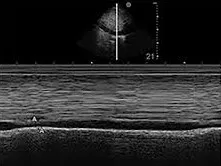
- Dilated small bowel loops: >2.5cm diameter[cite: 1].
- Peristalsis: Increased early; decreased or absent in late stages[cite: 1].
- Fluid-filled loops: “To-and-fro” movement of contents[cite: 1].
- Wall thickening: >3mm in ischemic cases[cite: 1].
- Transition point: Abrupt caliber change[cite: 1].
- Free fluid: Suggests strangulation[cite: 1].


2. Mechanical Large Bowel Obstruction (LBO)
Typically caused by carcinoma (60%), volvulus (15%), or diverticular disease (10%)[cite: 1]. Ultrasound has lower sensitivity than for SBO due to frequent gas distension[cite: 1].
Ultrasound Findings
- Colonic dilation: >6cm cecum, >8cm elsewhere[cite: 1].
- Haustral markings: Visible in distended colon[cite: 1].
- Peristalsis: Minimal or absent[cite: 1].
- Mass lesion: May be visible at the obstruction site[cite: 1].
- Pseudo-kidney sign: Common in annular lesions[cite: 1].
- Closed loop: Configuration seen in volvulus[cite: 1].


3. Paralytic Ileus
Functional obstruction due to impaired peristalsis without mechanical blockage, commonly postoperative or due to electrolyte imbalance, peritonitis, or medications[cite: 1].
Ultrasound Findings
- Diffuse bowel dilation: Affects both small and large bowel[cite: 1].
- Peristalsis: Absent or minimal—a key differentiating feature from mechanical obstruction[cite: 1].
- Fluid-filled loops: Static contents[cite: 1].
- No transition point[cite: 1].
- Wall thickness: Normal, unless secondary ischemia develops[cite: 1].

4. Closed Loop Obstruction
A surgical emergency where a bowel segment is obstructed at two points, often leading to volvulus and rapid progression to ischemia[cite: 1].
Ultrasound Findings
- U-shaped or C-shaped dilated loop: Converging ends are often visible[cite: 1].
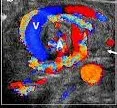
- Whirl sign: Twisted mesentery with swirling vessels (pathognomonic for volvulus)[cite: 1].
- Wall thickening: >4mm with loss of stratification[cite: 1].
- Mesenteric edema: Hyperechoic fat[cite: 1].
- Color Doppler: Absent signal in ischemic segments[cite: 1].

5. Comparative Ultrasound Features
| Feature | Mechanical SBO | Mechanical LBO | Paralytic Ileus | Closed Loop |
|---|---|---|---|---|
| Bowel Diameter | >2.5cm (small) | >6-8cm (colon) | Diffuse dilation | Localized U/C-shape |
| Peristalsis | Hyperperistalsis early | Minimal (normal) | Absent | Absent in loop |
| Transition Point | Present | Present | Absent | Two points |
| Wall Thickness | Normal (unless ischemic) | Normal (unless tumor) | Normal | Thickened (>4mm) |
| Key Sign | To-and-fro | Pseudo-kidney | Static fluid | Whirl sign |
:::tip Diagnostic Tip The combination of bowel loop configuration, peristalsis assessment, and presence/absence of a transition point allows reliable differentiation between obstruction types[cite: 1]. Always evaluate for signs of ischemia (wall thickening, absent flow, free fluid), which mandate urgent surgical intervention[cite: 1]. :::
References
- Taylor MR, Lalani N. Adult small bowel obstruction. Acad Emerg Med. 2013;20(6):528-544.
- Gottlieb M, et al. Utilization of ultrasound for the evaluation of small bowel obstruction: A systematic review and meta-analysis. Am J Emerg Med. 2018;36(2):234-242.
- O’Malley RG, et al. US of Gastrointestinal Tract Disease. Radiographics. 2015;35(1):50-68.
- Lal A, et al. Ultrasonography for the diagnosis of small bowel obstruction: a meta-analysis. ANZ J Surg. 2021;91(9):1748-1755.
- Khan R, et al. Role of ultrasonography in diagnosis of acute intestinal obstruction. J Pak Med Assoc. 2019;69(4):510-513.
- Catena F, et al. Bowel obstruction: a narrative review for all physicians. World J Emerg Surg. 2019;14:20.
- Rumack CM, Levine D. Diagnostic Ultrasound. 5th ed. Elsevier; 2018.
- American Institute of Ultrasound in Medicine (AIUM). AIUM practice guideline for the performance of gastrointestinal ultrasound examination. J Ultrasound Med. 2021;40(5):895-903.