Portal Hypertension: Ultrasound Diagnosis & Management
Portal hypertension is a clinical syndrome defined by a pathological increase in the portal venous pressure, with the hepatic venous pressure gradient (HVPG) exceeding 5 mmHg. Ultrasound plays a crucial role in the non-invasive assessment of portal hypertension, providing both direct and indirect signs of this condition.
Key Point: Ultrasound is often the first imaging modality employed when portal hypertension is suspected due to its non-invasive nature, lack of radiation, and ability to provide both critical anatomical and hemodynamic information.
Clinical Presentation
Patients presenting with advanced portal venous structural congestion typically display an array of secondary clinical symptoms:
- Ascites: The most common clinical manifestation of high pressure systemic back-flow.
- Gastroesophageal varices: Possesses a significant clinical risk of sudden, life-threatening hemorrhage.
- Splenomegaly: Progressive splenic enlargement stemming directly from chronic venous congestion.
- Hepatic encephalopathy: Neurocognitive shifts resulting from toxic systemic shunts bypassing normal hepatic clearance.
- Caput medusae: The visible engorgement and dilation of superficial periumbilical veins.
Ultrasound Findings
Direct Signs
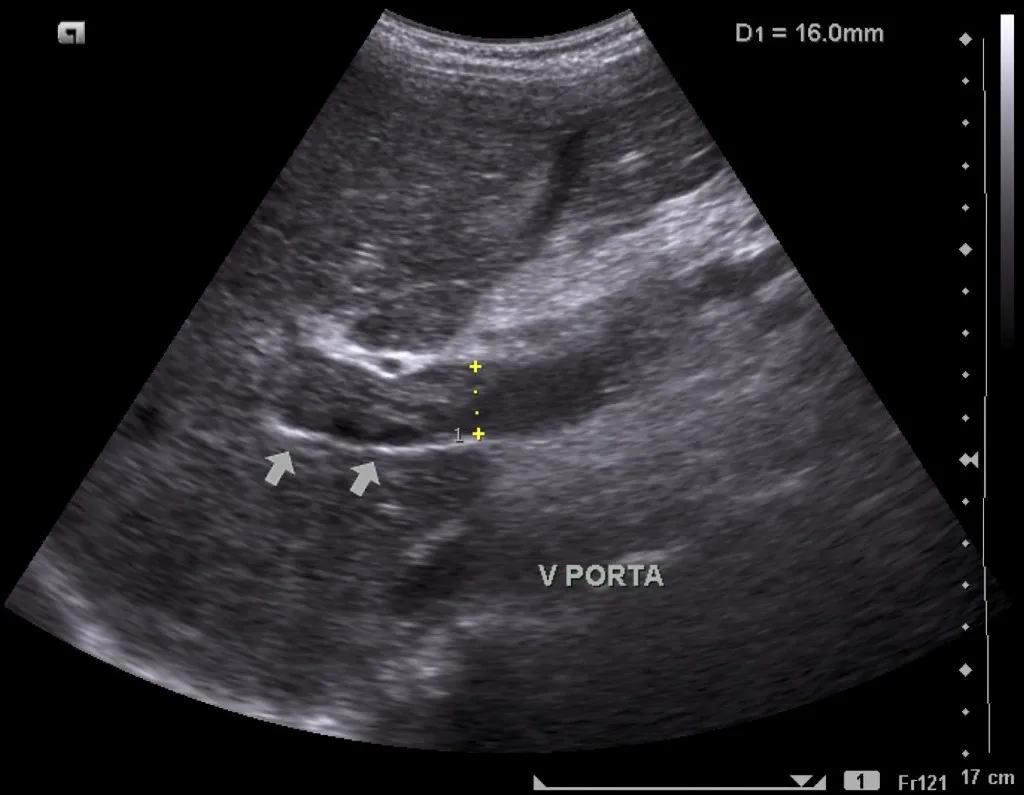
- Portal vein diameter greater than 13 mm: Measured reliably at the hepatic hilum during quiet, non-forced respiration.
- Loss of respiratory phasicity: Complete attenuation of respiratory variation in the portal vein Doppler waveform.
- Portal vein flow velocity less than 16 cm/s: Sluggish hepatopetal baseline velocity patterns.
- Hepatofugal flow: Pathological reversal of the portal vein flow stream moving away from the liver.
- Portal vein thrombosis: Partial or complete acoustic occlusion of the primary vessel lumen.
Indirect Signs
- Splenomegaly: Defined by a maximal longitudinal spleen length greater than 12 cm.
- Portosystemic collaterals (Varices):
- Paraumbilical vein recanalization within the ligamentum teres.
- Dilated coronary-gastric varices.
- Spontaneous splenorenal shunt pathways.
- Cavernous transformation: Network of periportal collateral vessels signaling chronic portal vein thrombosis.
- Ascites: Free fluid accumulation tracking within the dependent peritoneal recesses.
- Parenchymal changes: Increased echogenicity, surface nodularity, and structural changes consistent with baseline cirrhosis.
Imaging Case Gallery
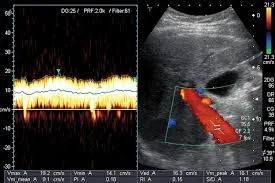


Diagnostic & Doppler Parameters
| Parameter | Normal Value | Portal Hypertension Presentation |
|---|---|---|
| Portal Vein Diameter | Less than 13 mm | Greater than 13 mm |
| Portal Vein Velocity | 16 to 40 cm/s | Less than 16 cm/s |
| Congestion Index (Area/Velocity) | Less than 0.07 | Greater than 0.07 |
| Flow Direction Profile | Hepatopetal (Toward liver) | Hepatofugal (Away from liver) in advanced configurations |
Collateral Pathways
As vascular resistance inside the liver parenchymal framework rises, the portal system selectively decompresses through several classic primitive embryonic portosystemic collateral routes:
- Gastroesophageal varices: Located around the gastric cardia and lower esophagus; bears the highest clinical priority for catastrophic rupture.
- Paraumbilical vein: Recanalization of the ligamentum teres, presenting as a tortuous vascular route tracking from the left portal vein directly to the anterior abdominal wall.
- Splenorenal shunts: Large, abnormal vascular communications developing naturally between the splenic vein and the left renal vein.
- Hemorrhoidal plexus: Structural pressure offloading linking superior hemorrhoidal paths with systemic middle or inferior rectal veins.
Conclusion
Ultrasound remains an invaluable, highly repeatable first-line tool for assessing the portal venous network. By synthesizing grayscale structural observations with spectral Doppler hemodynamic waveforms, clinicians can reliably identify portal hypertension, map life-threatening collateral variants, and monitor long-term therapeutic interventions non-invasively.
References
- Berzigotti A, et al. Ultrasound in portal hypertension - part 1. Ultraschall Med. 2021;42(1):34-57.
- Dietrich CF, et al. Ultrasound in portal hypertension - part 2. Ultraschall Med. 2021;42(2):128-161.
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines for the management of patients with portal hypertension. J Hepatol. 2018;69(4):716-735.
- American College of Radiology. ACR Appropriateness Criteria: Radiologic Management of Portal Hypertension. Updated 2022.