Fetal Doppler Ultrasound Scan
Introduction
• Doppler ultrasound = measures blood flow in fetal and maternal vessels
• Non-invasive, safe, widely used in obstetrics
• Helps assess fetal well-being and placental function
Learning Objectives
By the end of this session, health workers should:
- Understand principles of Doppler ultrasound
- Identify common indications for use in pregnancy
- Recognize key vessels assessed
- Interpret basic findings
- Apply Doppler in antenatal care for better outcomes
Principles of Doppler Ultrasound
- Based on Doppler effect: frequency change of sound waves from moving blood cells. We detect speed and direction.
Modes of Doppler Ultrasound:
- Continuous Wave
- Pulsed Wave
- Color Doppler: Converts blood flow into colors overlaid on an image to show speed and direction.
- Spectral Doppler: Displays blood flow as a graphical wave measuring exact velocity, allowing doctors to listen to the flow as an audible pulse.
- Power Doppler: A more sensitive technique used to detect low blood flow in smaller, deeper vessels

Figure 1: Dual-panel fetal ultrasound image demonstrating a normal, coiled 3-vessel umbilical cord. The left panel uses color Doppler (CF) to illustrate direction-dependent blood flow with alternating red and blue signals. The right panel employs color power angiography (CPA) to highlight the continuous vascular structure and perfusion in a uniform orange-gold hue.
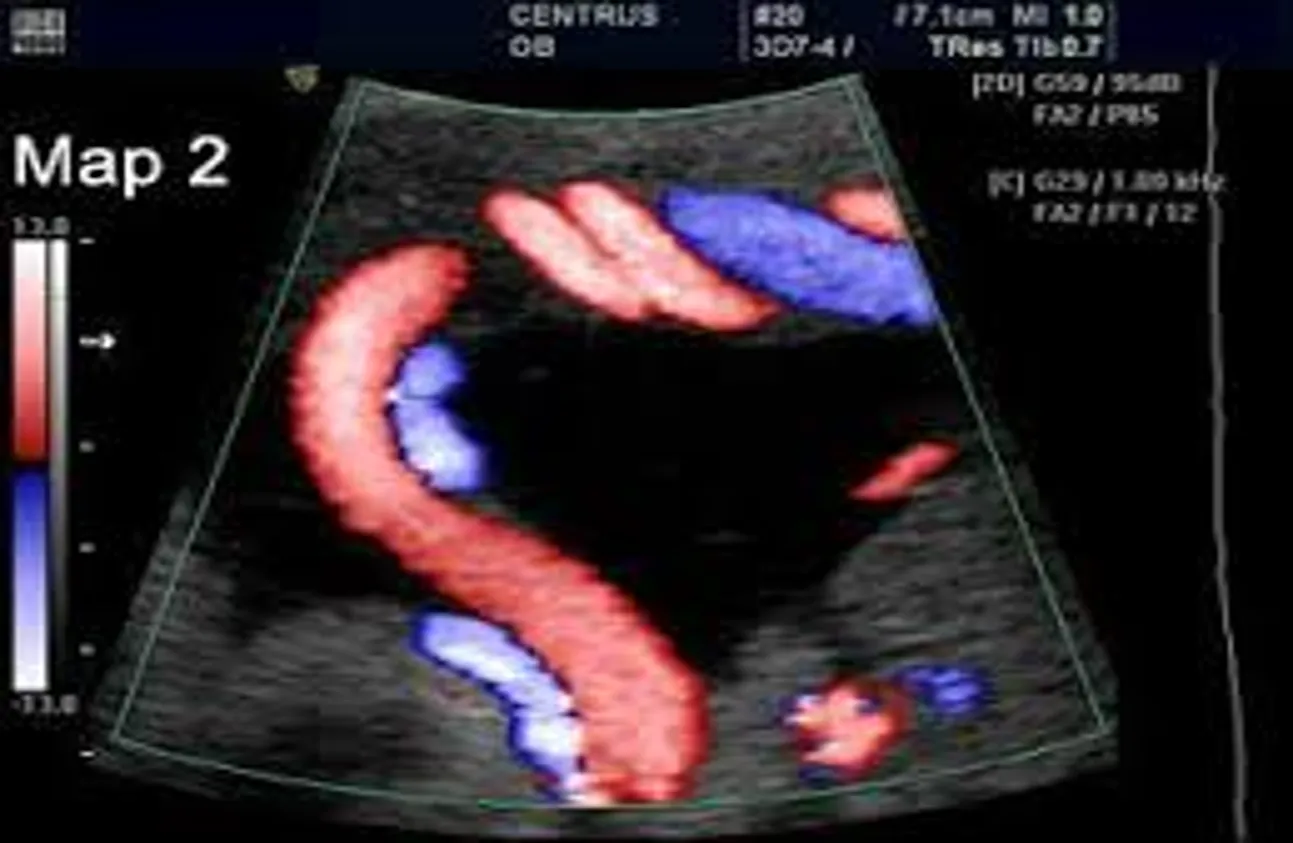
Figure 2: Color Doppler ultrasound image showing blood flow within umbilical vessels, with red and blue colors indicating the direction of movement.
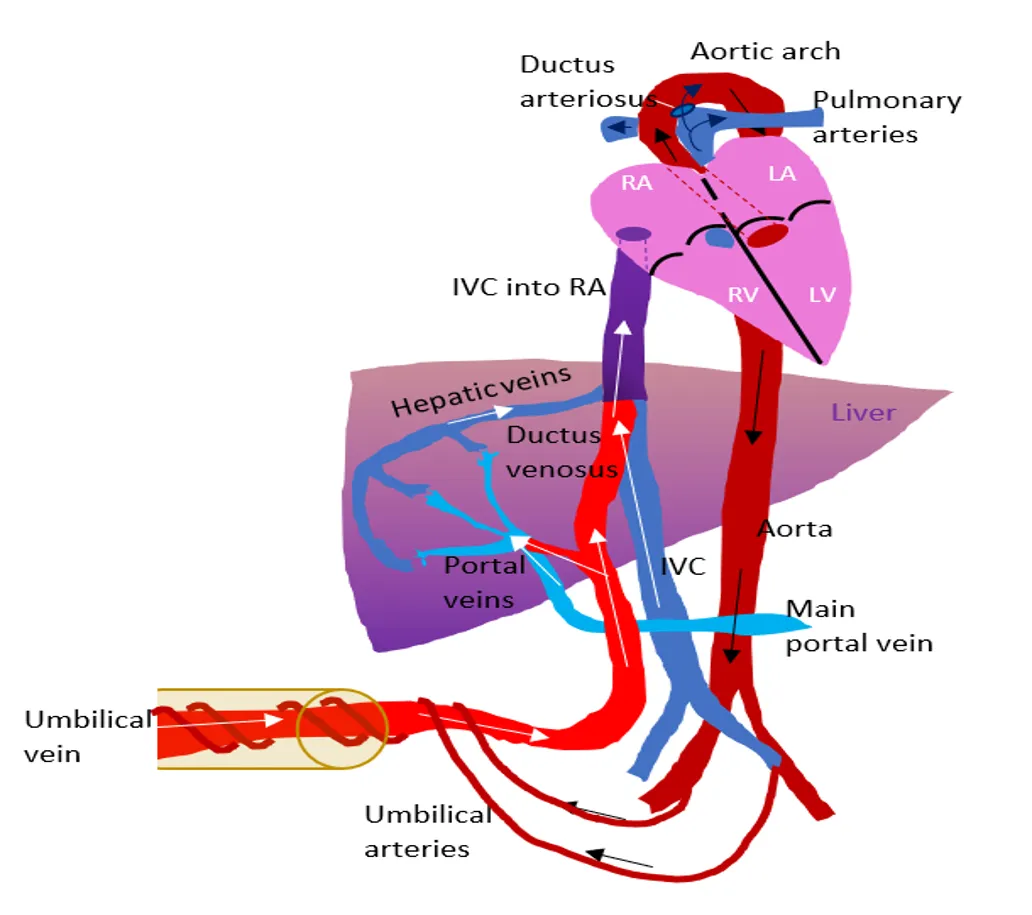
Figure 3: Simplified anatomical diagram showing the pathways of fetal circulation. The illustration highlights how blood moves from the umbilical vessels through shunts like the ductus venosus and ductus arteriosus to bypass the non-functional fetal lungs.
Indications in Obstetrics
- Suspected intrauterine growth restriction (IUGR)
- Hypertensive disorders (pre-eclampsia, eclampsia)
- Monitoring high-risk pregnancies (diabetes, anemia, twins)
- Assessment of fetal hypoxia and well-being
- Evaluation of placental function, e.g. post trauma
Key Vessels Assessed
- Umbilical artery → placental resistance
- Middle cerebral artery (MCA) → fetal brain oxygenation
- Ductus venosus → cardiac function
- Uterine arteries → maternal circulation & risk of pre-eclampsia

Normal vs Abnormal Findings
- Umbilical artery:
- Normal: low resistance, forward flow
- Abnormal: absent/reversed end-diastolic flow → fetal compromise
- MCA:
- Low resistance suggests ‘brain-sparing’ effect (fetal hypoxia)
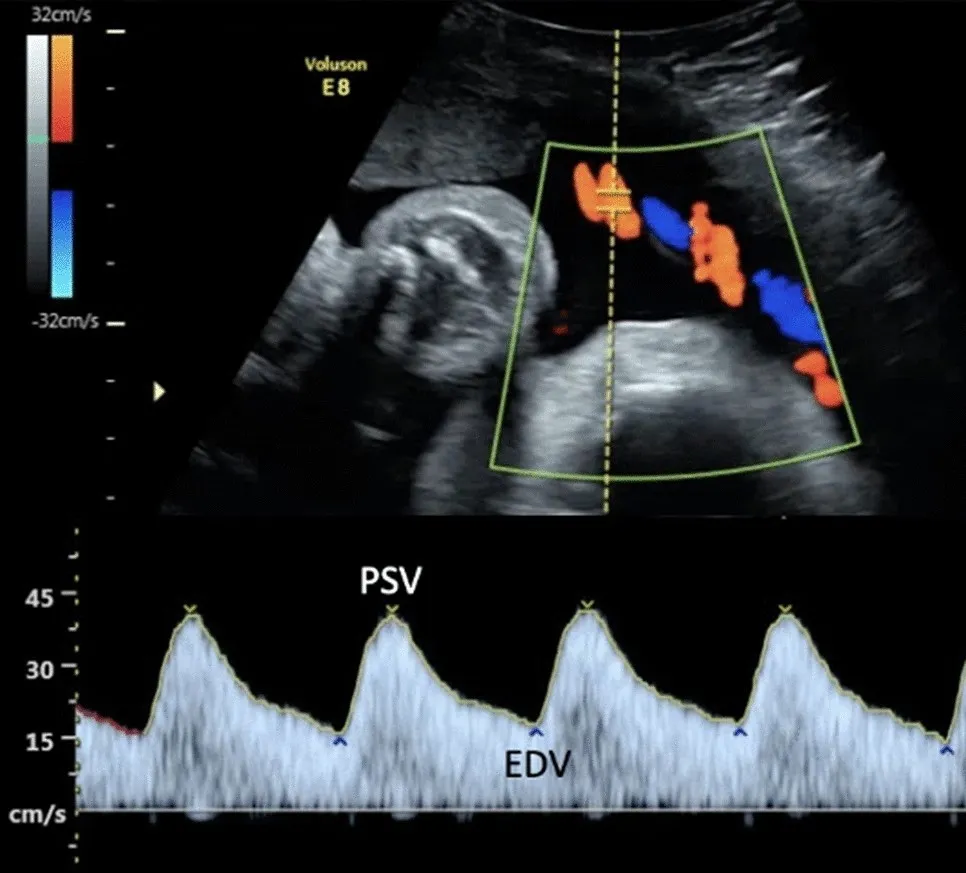
Umbilical artery normal Doppler sampling: Spectral Doppler ultrasound scan showing normal umbilical artery blood flow sampling. The top image maps the target vessel, while the bottom waveform graphs blood velocity over time, highlighting the Peak Systolic Velocity (PSV) and End-Diastolic Velocity (EDV).
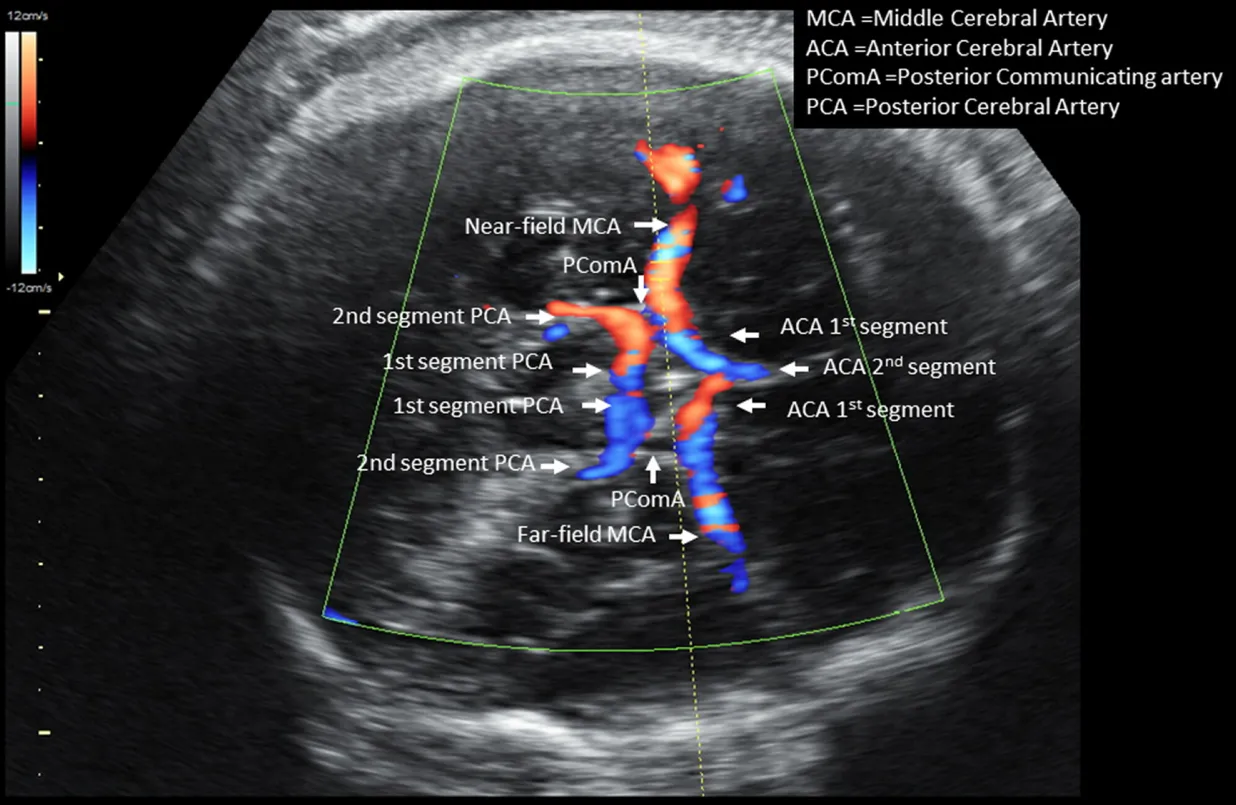
Fetal middle cerebral artery at circle of Willis: Color Doppler ultrasound displaying blood flow within the fetal cranial arteries, including the middle, anterior, and posterior cerebral arteries.
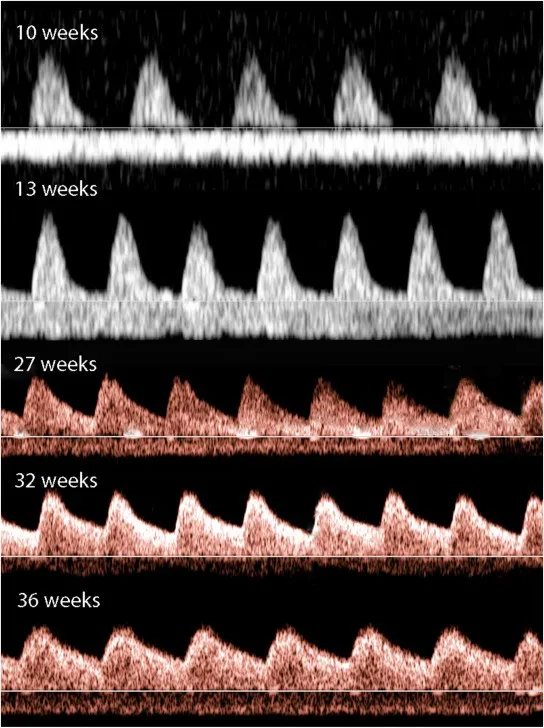
Variation of Umbilical artery Doppler with GA: Spectral Doppler waveforms showing the normal evolution of umbilical artery blood flow from 10 to 36 weeks of gestation, demonstrating a progressive increase in end-diastolic flow over time.
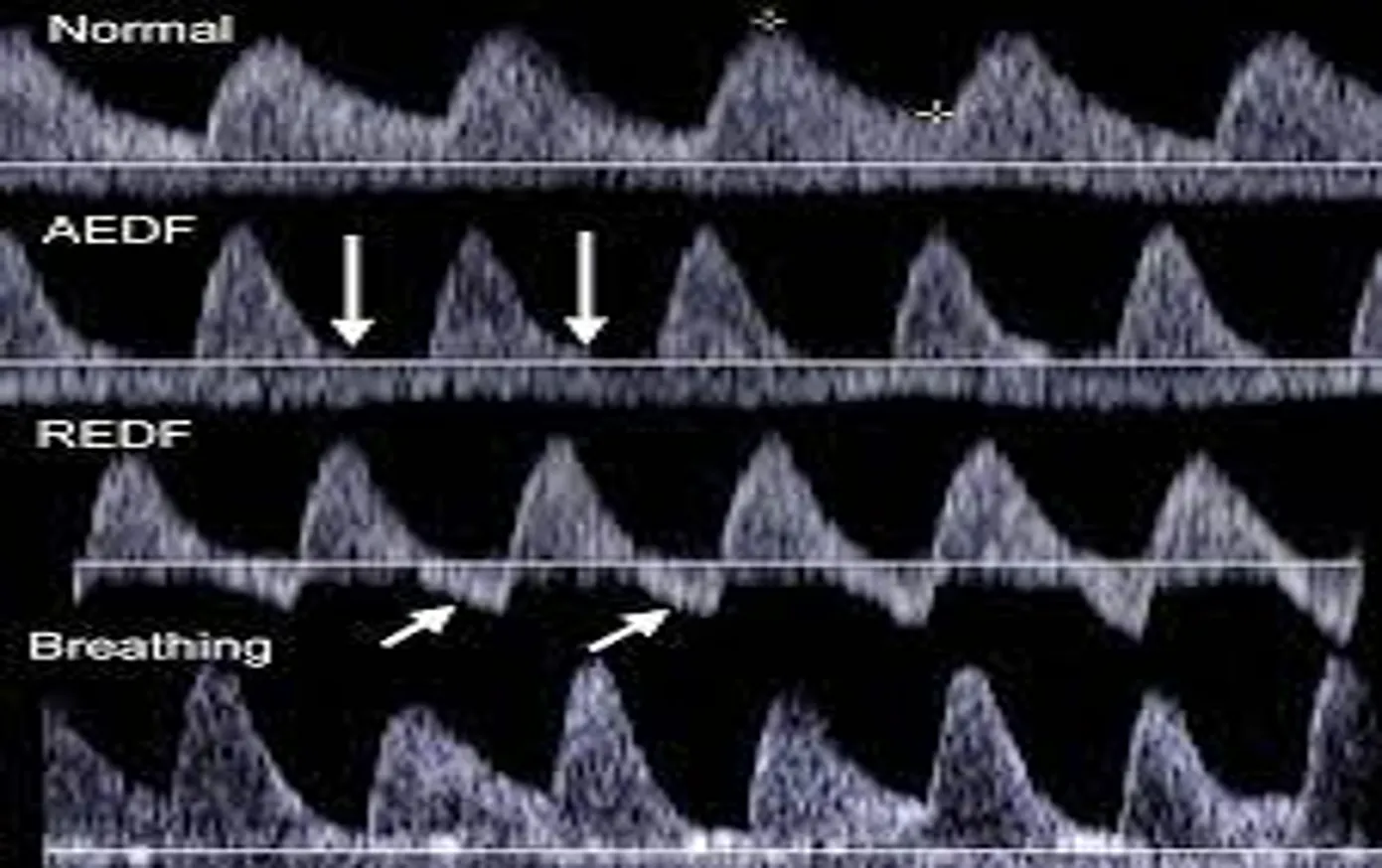
Umbilical Artery Doppler Waveforms: Spectral Doppler ultrasound panels showing normal umbilical artery flow compared to abnormal states: Absent End-Diastolic Flow (AEDF), Reversed End-Diastolic Flow (REDF), and waveform distortion caused by fetal breathing movements.
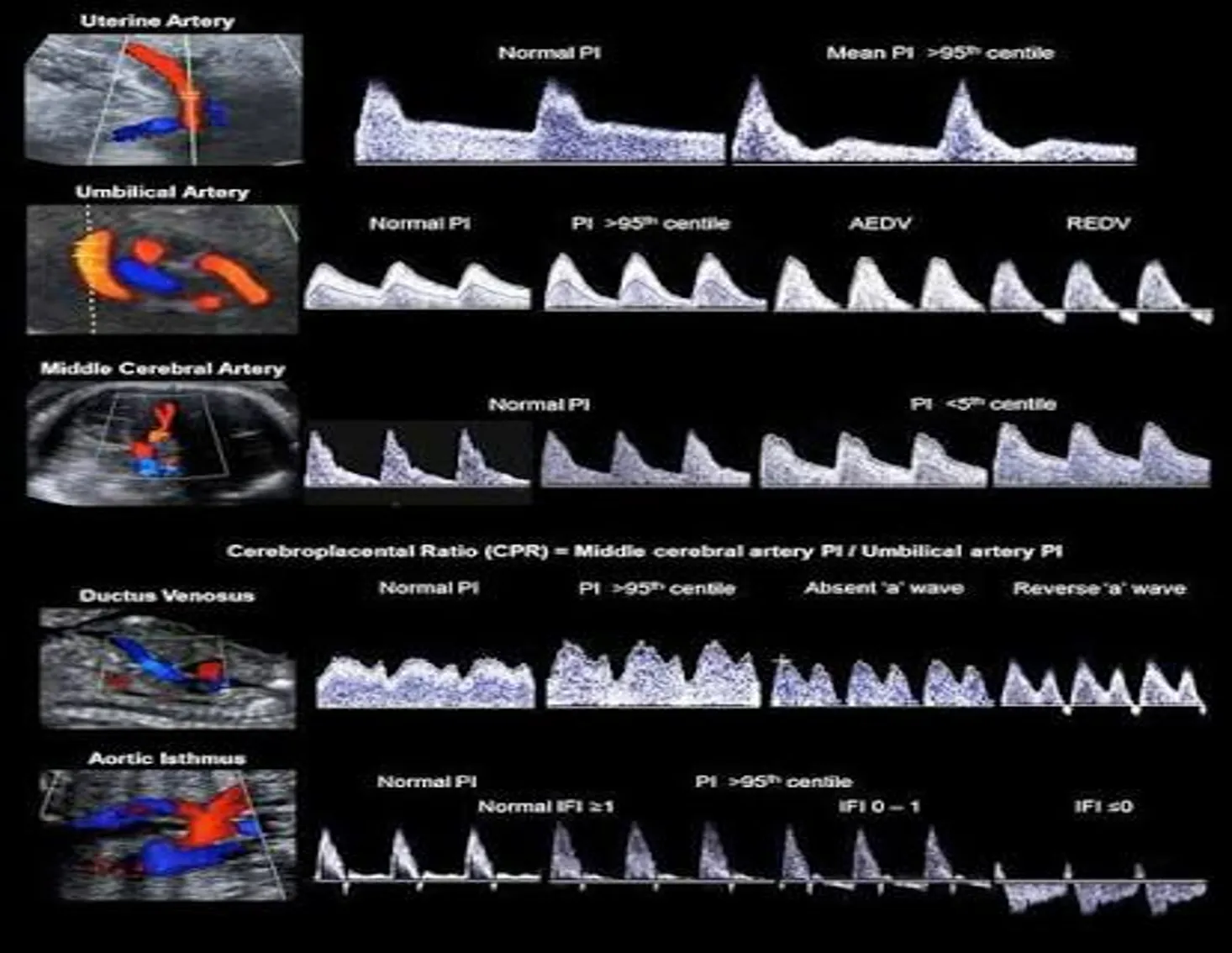
Reference chart combining color and spectral Doppler ultrasound images to show normal versus abnormal blood flow waveforms across key maternal and fetal vessels (uterine artery, umbilical artery, MCA, ductus venosus, and aortic isthmus), including the formula for the Cerebroplacental Ratio (CPR).
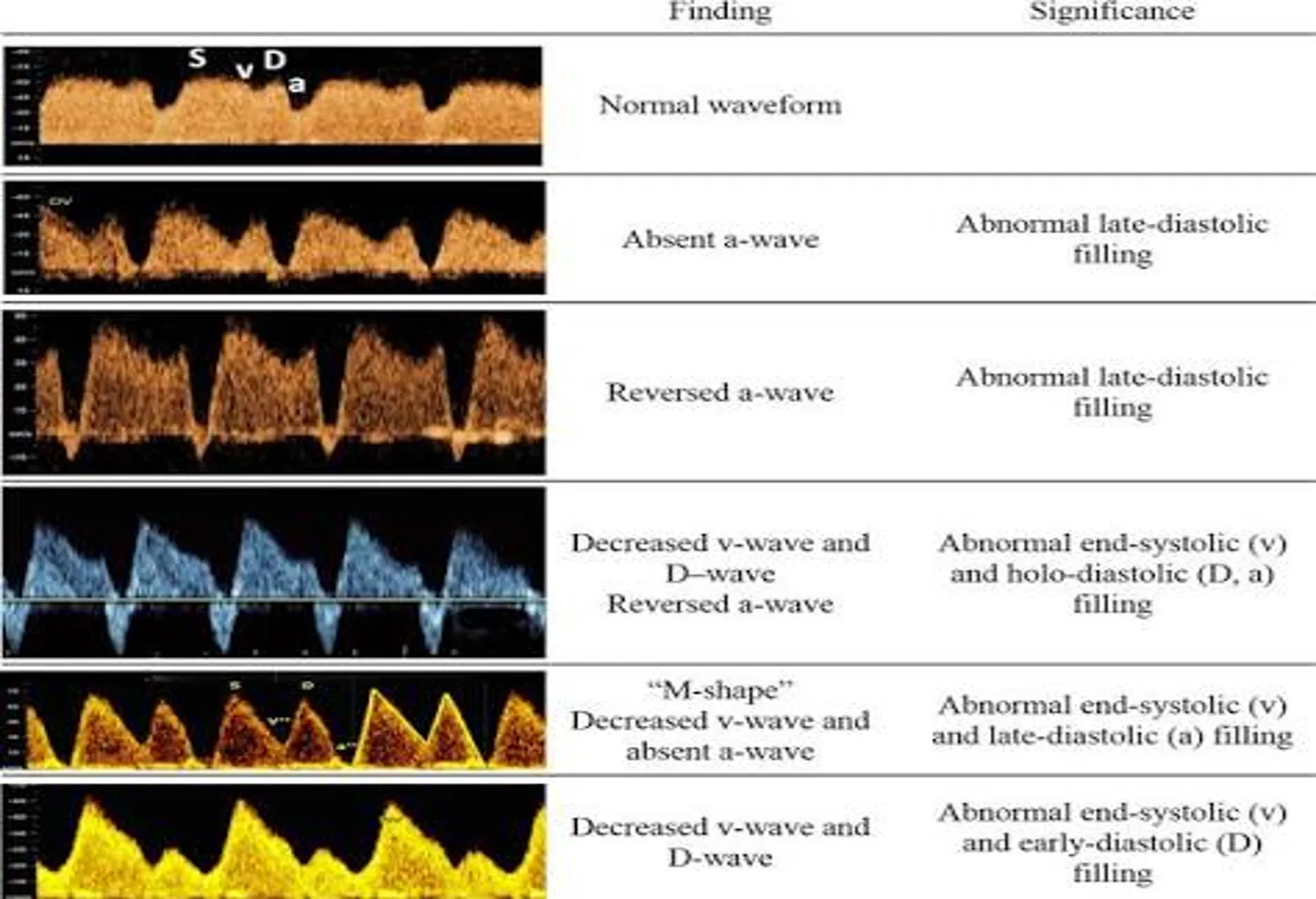
Ductus venosus: Reference table showing spectral Doppler ultrasound waveforms. The chart details normal waveforms alongside abnormal variations (such as absent or reversed a-waves) to assess fetal cardiac and venous filling functions.
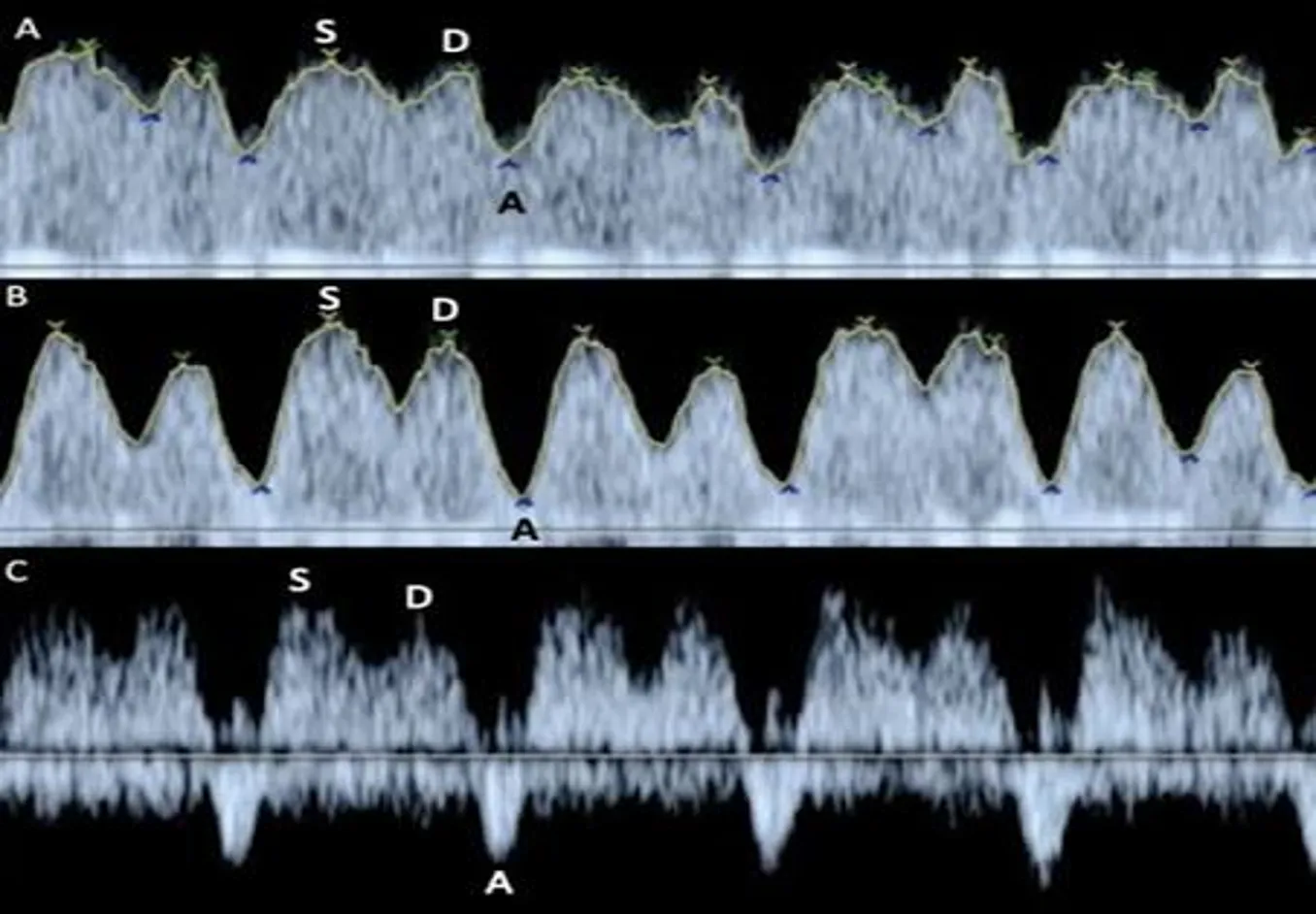
Fetal ductus venosus: TSpectral Doppler ultrasound panels showing three different venous flow waveforms (labeled A, B, and C). The graphs track ventricular systole (S), early diastole (D), and atrial contraction (A) to evaluate progressive changes in fetal venous hemodynamics.
Clinical Importance
- Early detection of fetal compromise
- Guides timing of delivery in high-risk pregnancies
- Reduces risk of stillbirth or complications e.g. ventricular hemorrhage, cerebral edema, CP
- Complements other tests (NST, BPP, growth scans)
Limitations
- Operator-dependent
- Requires proper training & equipment
- Not useful as routine screening for all low-risk pregnancies
- Interpretation may vary
Role of Health Workers
- Identify high-risk mothers
- Refer for Doppler scans when indicated
- Counsel mothers on importance of follow-up
- Collaborate with obstetricians for management
Case Example
- Mother: 28 years, 34 weeks, pre-eclampsia
- Doppler: Umbilical artery – absent end diastolic flow
- Decision: Close monitoring + consider early delivery
Summary
- Fetal Doppler = essential tool for monitoring high-risk pregnancies
- Main vessels: Umbilical artery, MCA, Ductus venosus, Uterine arteries
- Helps reduce maternal and perinatal morbidity/mortality
- Health workers play a key role in screening, referral, and follow-up
References
- WHO. Recommendations on Antenatal Care.
- American College of Obstetricians and Gynecologists (ACOG)
- Campbell S, et al. Doppler Ultrasound in Obstetrics