Ultrasound Case: Benign Prostate Hyperplasia with Rectal Compression
Clinical History
A 70-year-old male presented to the outpatient clinic with complaints of progressive difficulty in passing stool over the past several months. The patient described a sensation of incomplete bowel evacuation and occasional straining during defecation. There was no history of constipation related to dietary changes, no rectal bleeding, and no weight loss.
The patient denied any urinary symptoms, including dysuria, frequency, urgency, nocturia, or weak urinary stream. There was no history of urinary retention or previous urological conditions.
On physical examination, the abdomen was soft and non-tender with no palpable masses. Digital rectal examination (DRE) revealed a markedly enlarged, smooth, and firm prostate bulging into the anterior rectal wall, causing apparent narrowing of the rectal lumen.
Ultrasound Findings
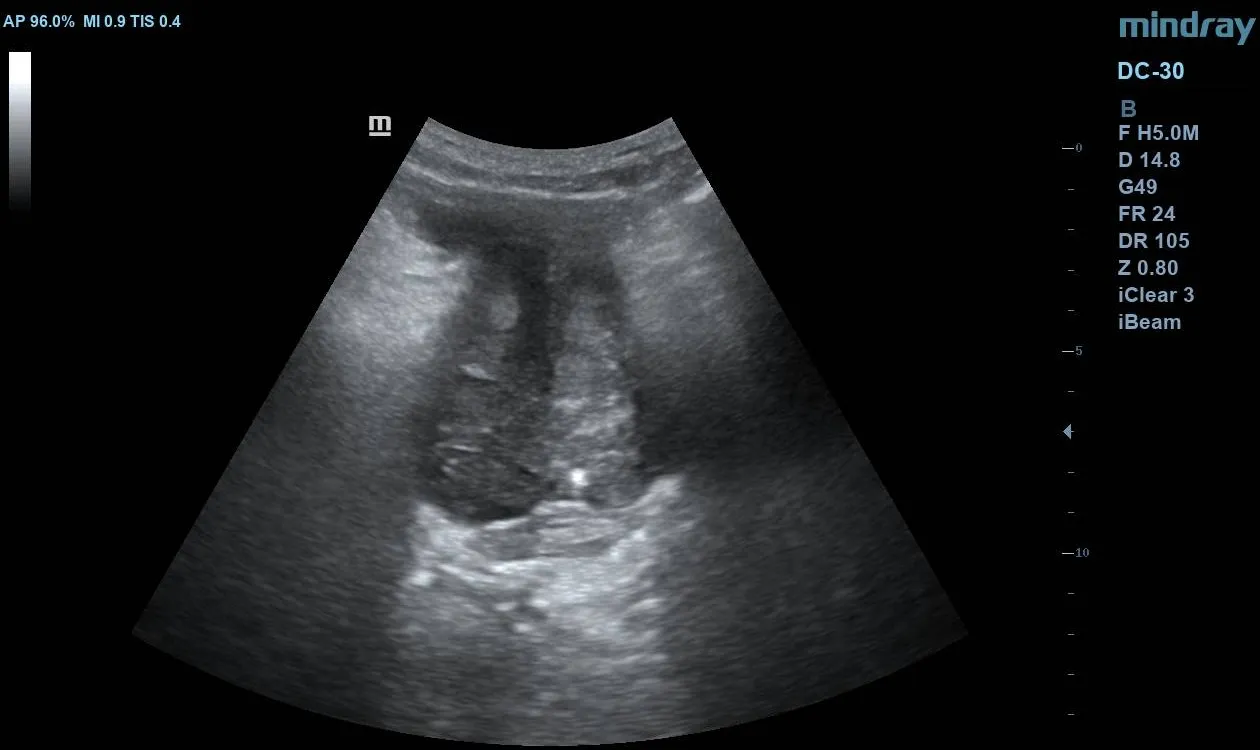
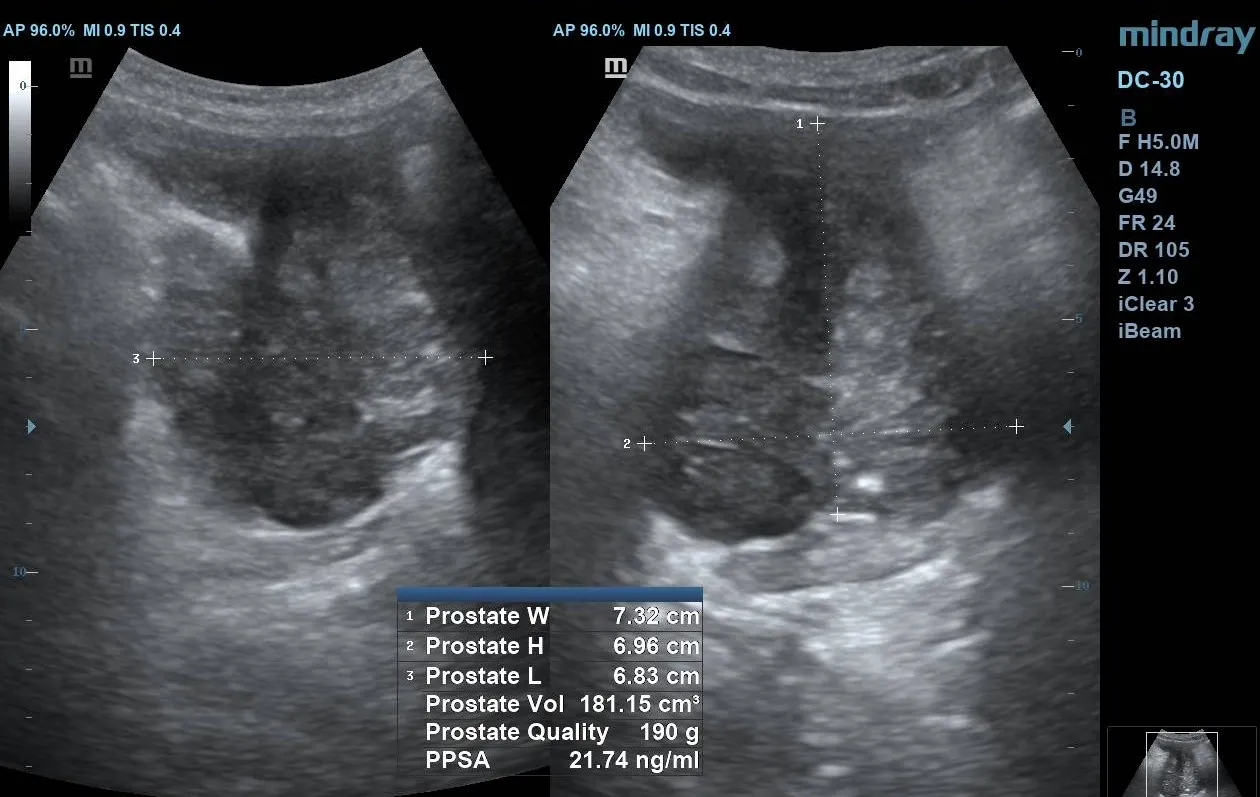
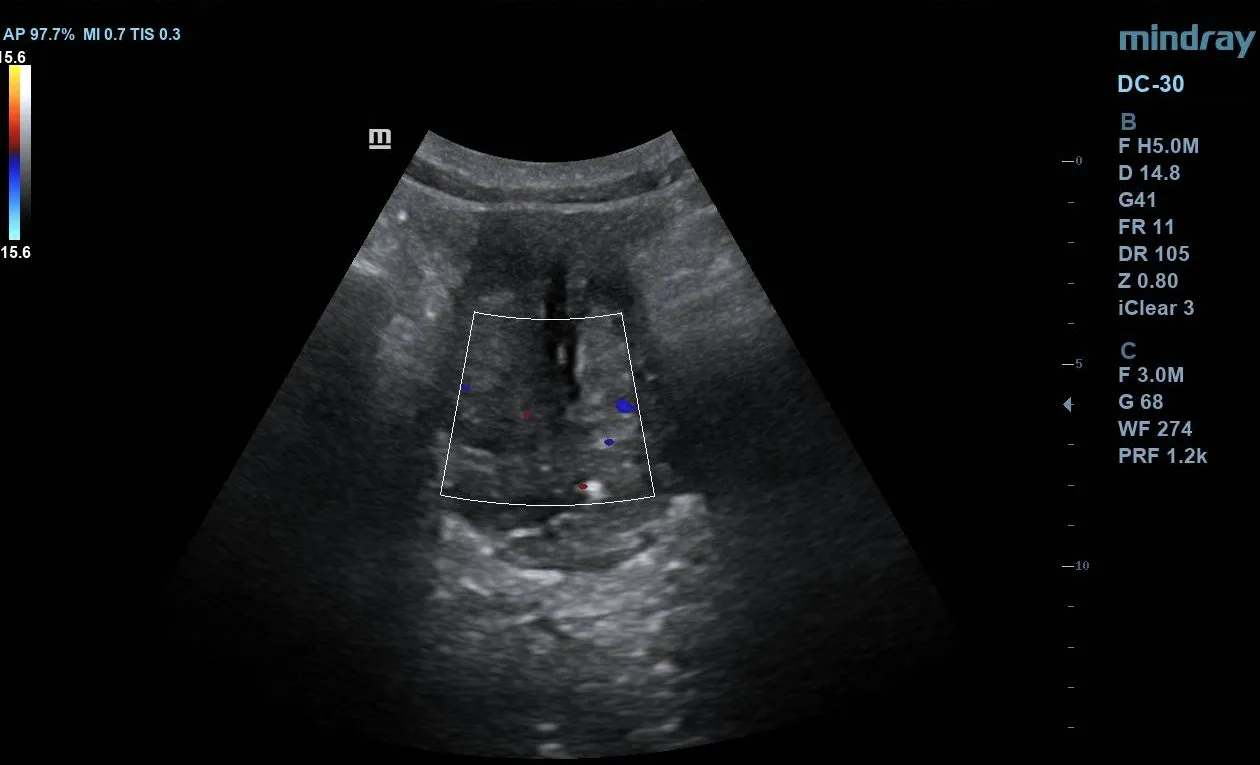
Pelvic ultrasound evaluation revealed:
- A markedly enlarged prostate gland with an estimated volume of 181.15 mL (significantly above the normal range of 20–30 mL).
- Predominantly homogeneous but mildly heterogeneous echotexture with nodular enlargement, mainly involving the transitional zone.
- A rounded gland contour with smooth outer margins.
- Prominent median lobe enlargement projecting into the bladder base, causing mild indentation of the inferior bladder wall.
- Significant posterior mass effect on the anterior rectal wall, contributing to narrowing of the rectal lumen.
- The urinary bladder appeared decompressed at the time of examination.
Additional Findings
- Further imaging with pelvic CT (if performed) would typically demonstrate mass effect of the enlarged prostate on the rectum, explaining the patient’s bowel-related symptoms.
- Laboratory investigations, including prostate-specific antigen (PSA), were within acceptable range for age, with no immediate suspicion of malignancy.
Discussion
This case represents an atypical manifestation of benign prostate hyperplasia (BPH). While urinary symptoms dominate most clinical presentations, the prostate’s anatomical proximity to the rectum means that significant enlargement can exert pressure posteriorly, leading to bowel-related symptoms such as constipation or difficulty in stool passage.
The absence of urinary symptoms in this case is particularly notable, highlighting that bladder outlet obstruction is not always present even in significantly enlarged prostates.
Management
The patient was managed conservatively with a combination of:
- Alpha-blockers to reduce prostatic smooth muscle tone
- Stool softeners and dietary modifications
- Monitoring for development of urinary symptoms
In cases where symptoms persist or worsen, surgical intervention such as transurethral resection of the prostate (TURP) may be considered.
Differential Diagnosis
Although imaging findings are consistent with BPH, other considerations may include:
- Prostate carcinoma (typically associated with irregular margins, focal lesions, and elevated PSA)
- Rectal masses causing secondary compression
- Pelvic masses of non-prostatic origin