Ultrasound Case: Hashimoto's Thyroiditis
A 42-year-old female presents with neck swelling, localized discomfort, and systemic fatigue.
Case Presentation
History
- Chief Complaint: Neck discomfort and profound fatigue x 3 weeks.
- History of Present Illness:
- Gradual onset of anterior neck swelling and mild subjective tenderness.
- Mild intermittent dysphagia to solids; no history of odynophagia or respiratory compromise.
- Generalized fatigue, cold intolerance, and unexpected weight gain (4kg over the past 3 weeks).
- No recent history of spikes in fever, chills, upper respiratory infections, or preceding viral illnesses.
- Past Medical History: Significant maternal family history of primary hypothyroidism (affecting mother and sister).
- Medications: None.
Physical Examination
- Neck Examination: Diffusely enlarged, symmetric thyroid gland (~2x normal size); firm on palpation with mild, non-exquisite tenderness; moves freely upon deglutition.
- Lymphatic Profile: No cervical, supraclavicular, or localized lymphadenopathy detected.
- Vital Signs: BP 120/80 mmHg, HR 68 bpm (bradycardic trend), Temp 36.8°C.
Initial Laboratory Findings: Markedly elevated TSH at 8.2 mIU/L (normal: 0.4–4.0 mIU/L); reduced Free T4 at 0.8 ng/dL (normal: 0.9–1.7 ng/dL); strongly positive Anti-TPO antibodies >600 IU/mL; mildly elevated ESR at 22 mm/hr. These lab values strongly match primary hypothyroidism secondary to autoimmune chronic lymphocytic thyroiditis.
Ultrasound Findings
- Marked Parenchymal Heterogeneity: Diffuse coarsening of the thyroid parenchyma interspersed with numerous tiny, ill-defined micronodules ranging between 1–6mm.
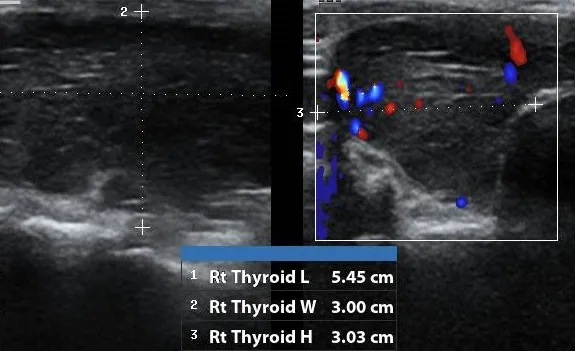
- Diffusely Hypoechoic Echogenicity: The entire thyroid gland displays significantly reduced echogenicity when structurally compared directly to the adjacent anterior strap muscles.
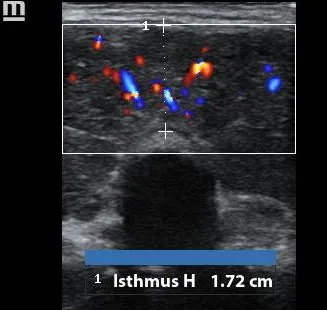
- Hypervascularity (“Thyroid Inferno”): Color and power Doppler parameters demonstrate a diffuse, intense increase in intra-parenchymal blood flow pattern during the active inflammatory stage.
- Thyromegaly with Isthmus Dilation: Bilateral lobe enlargement with the midline thyroid isthmus tracking well past normal thresholds at 17.2mm (1.72cm).
- Reactive Lymph Nodes: Visualized regional cervical lymph nodes display normal oval morphology and a preserved fatty hilum, indicating a benign reactive state.

Final Diagnosis: Hashimoto’’s Thyroiditis (Chronic Lymphocytic Thyroiditis)
Confirmed by correlating the clinical features of secondary hypothyroidism with characteristic transabdominal ultrasound markers (diffuse hypoechogenicity, micronodularity, isthmic hypertrophy) and strongly positive serum anti-thyroid peroxidase (TPO) antibodies.
Differential Diagnosis
- Subacute Granulomatous Thyroiditis (de Quervain): Presents with an acutely painful, exquisite neck mass typically following a viral upper respiratory infection. Ultrasound reveals poorly defined, geographic focal hypoechoic areas that migrate over time and display transient “washout” avascularity rather than diffuse micronodularity; clinically supported by a highly elevated ESR (>50 mm/hr).
- Graves’’ Disease: Shares a similar hypervascular “thyroid inferno” pattern and diffuse hypoechogenicity on ultrasound. However, it characteristically lacks the fine micronodular parenchymal scarring found in Hashimoto’’s and is clinically distinguished by overt clinical hyperthyroidism (anxiety, tachycardia, exophthalmos) and positive TSH-receptor antibodies (TRAb).
- Benign Multinodular Goiter (MNG): Features multiple discrete, asymmetric adenomatous nodules varying in echogenicity and cystic degeneration. Differentiated easily on ultrasound by the presence of completely normal, unaltered intervening thyroid parenchyma separating the distinct focal nodules.
- Acute Suppurative Thyroiditis: A rare bacterial infection presenting with high leukocytosis, localized fluctuating erythema, and severe severe unilateral pain. Sonography demonstrates a focal, liquid-debris filled hypoechoic abscess collection within a single lobe rather than a uniform, symmetric systemic disease.